General medicine case 1
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here, we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs
A 45 yr old patient presented to the opd with the chief complaint of fever , loose stools 20 episodes , vomiting 20 episodes since 1 month
HISTORY OF PRESENT ILLNESS
Patient was apparently asymptomatic 6 months back. Then the patient complaints of fever which is intermittent
Loose stools - large volume; watery in consistency not with any mucus or blood and no abdomen pain
vomiting- non projectile ; contains food particles and non foul smelling
- Fever ; vomiting; sudden weight loss since 2 months and also complaints of loss of appetite
- lt all started 6 months back, when the patient had complaint of fever she visited a medical health care centre and treatment was taken.Then the patient was fine for 2 months.
- After 2 months the patient had fever ; weight loss and then visited diagnostic centre, reports were normal then the patient was fine for 15 days
- On 26/07/21 - patient had vomiting ; loose stools and fever then the patient visited hospital treatment was taken and used tablets for 5 days
- On 31/07/21- patient was fine
- On 7/08/21- patient comes to the opd with similar complaints and weakness in general
HISTORY OF PAST ILLNESS
There is no history of diabetes mellitus; Hypertension; asthma; tuberculosis; epilepsy
There is history of blood transfusion 16 years back due to hysterectomy due to blood loss
PERSONAL HISTORY
- Diet is mixed
- Decreased appetite
- loose stools since 15 days
- No addictions
FAMILY HISTORY
-No history of similar complaints in the family
GENERAL EXAMINATION
Patient is conscious, coherant , co-operative. She is well oriented to time , place and person
No anemia
No pallor
No cyanosis
No clubbing
No generalized lymphadenopathy
No pedal edema
Vitals
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM
Inspection:
Chest wall is bilaterally symmetrical
No Precordial bulge
No visible pulsations, engorged veins,scars, sinuses
Palpation:
JVP - normal
Apex beat : felt in the left 5th intercostal space
In midclavicular line
Ausculation:
S1 ,S2 Heard
RESPIRATORY SYSTEM
Bilateral airway +
Position of trachea- central
Normal vesicular breath sounds - heard
No added sounds
PER ABDOMEN
Abdomen is soft and non tender
Bowel sounds heard
No palpable mass or free fluid
CENTRAL NERVOUS SYSTEM
Patient is conscious
Reflexes are normal
Speech is normal
PROVISIONAL DIAGNOSIS
Acute gastroenteritis?
INVESTIGATION
Oral manifestation:- white patch

Hemogram:

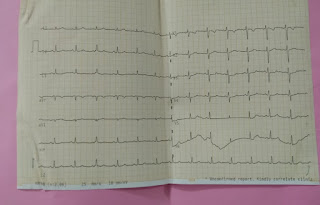
ECG:



Blood urea:

FINAL DIAGNOSIS
HIV positive
TREATMENT
On 07/08/2021

{kind=link}
Comments
Post a Comment