General medicine case 4
HISTORY OF PRESENT ILLNESS
Patient was apparently asymptomatic 45 days back. Then the patient developed shortness of breath which is grade 3 since 20 days and leg pain since 20 days there is history of trauma of his left leg 3 months back.complaints of pitting type of edema involving left leg.
Patient had fever 2 months back which subsided on medication
Patient complaints of fever which is intermittent and cough since 3 to 4 days . patient also complaints of tiredness and weakness. Patient is unable to walk . There is no history of body pains on 13th September 2021
HISTORY OF PAST ILLNESS
There is no history of hypertension, diabetes mellitus , tuberculosis, asthma, and epilepsy
There is history of blood transfusion (4 units ) Suryapet 10 days back
PERSONAL HISTORY
Diet is mixed , vegetarian
Sleep is adequate
Bowel and bladder movements are regular
Appetite is normal
There is no history of allergies to known drugs
Patient was drinking alcohol occasionally 4 yrs back then stopped drinking
He is married and has 2 children
FAMILY HISTORY
There is no history of similar complaints in the family members
GENERAL EXAMINATION
The patient is conscious, coherant and cooperative. He is well oriented to time , place and person . Moderately built and nourished
Anemia present
Pallor present
No icterus
No cyanosis
No clubbing
No generalized lymphadenopathy



VI
Vitals
PR 90bpm
RR 17cpm
BP 110/70mmHg
SpO2 98% in room air
GRBS 159mg/dl
Temperature febrile
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM
Inspection:
Chest wall is bilaterally symmetrical
No Precordial bulge
No visible pulsations, engorged veins,scars, sinuses
Palpation:
JVP - normal
Apex beat : felt in the left 5th intercostal space
In midclavicular line
Ausculation:
S1 ,S2 Heard
RESPIRATORY SYSTEM
Bilateral airway +
Position of trachea- central
Normal vesicular breath sounds - heard
No added sounds
PER ABDOMEN
Abdomen is soft and non tender
Bowel sounds heard
No palpable mass or free fluid
CENTRAL NERVOUS SYSTEM
Patient is conscious
Reflexes are normal
Speech is normal
PROVISIONAL DIAGNOSIS
Pancytopenia under evaluation
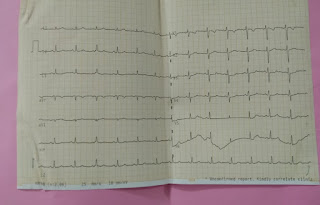
INVESTIGATIONS















TREATMENT
1. Inj METHYLCOBALAMINE 1000mg IV OD
2. Inj IRON SUCROSE 1 amp in 100ml NS IV
3. Vitals monitoring
Bone marrow aspiration and biopsy was done in the afternoon .
On 16th September
Patient had 2 episodes of vomiting ,and suddenly became breathless ,with profuse sweating ,cold peripheries ,feeble pulse ,BP -80/60 mmHg
Spo2 on room air -52 %
RR-38/ min HR-110/ min
RS- Bae+ , clear CVs -s1,S2 heard no murmurs .
ABG - severe metabolic acidosis - PH-7.2 Hco3-5
Paco2- 9.2
Assessment- septic shock ? / Cardiogenic shock ?
Heart failure Severe anemia
Plan - O2 inhalation Ionotropic support- on noradrenaline .
Started on Piptaz
PRBC transfusion
( Informed to first on call sir on duty ) .
On 16th September Patient was declared as death

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments
Post a Comment