General medicine case 9
This is an online e-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs
A 50 old yr female patient she is House wife presented to opd with chief complaints of shortness of breath 10 days back
HISTORY OF PRESENT ILLNESS
Patient was apparently asymptomatic 9 yrs back then she had fever visited to local hospital and blood investigations were done she was diagnosed with Diabetes mellitus and hypertension and she has been taking medication for DM and hypertension since 9 yrs
On 6th March 2021 she was noticed pedal edema which was pitting type and gradual on onset and at that time she came to opd in semiconscious state and with profuse sweating and she was discharged from our hospital 11th March
she had pedal edema 6 months back and facial puffiness on and off 2 months back and cough since 3 months shortness of breath 2 months back which aggrevated since 10 to 15 days back presented to opd on chief complaint of shortness of breath on rest since 10 days back she was admitted the on 8th December 2021 they came back to hospital and decreased urine output since 1 and half month and attender constantly saying that she used to have giddiness and fell down due to hypoglycemia
Daily routine before illness:- she used to wake up a 4 o clock in the morning do her household work and pack tiffin for her children she used to have breakfast by 10 that is rice and dal then she used to have her lunch by 2 then go farm she was daily wage labourer she used to work in paddy field like sowing the seeds, harvesting and come back to home by 6 then she used to prepare dinner for family members then have the dinner by 8 or 9
Daily routine after illness :- inspite of her weakness she used to do all her household work since 1 yr she is not going to paddy field she stopped working
PERSONAL HISTORY
Diet is mixed
She had loss of appetite 6 months back then presently her appetite is normal
Bladder movements decreased urine output since 1and half month
Bowel movement regular
Addictions :- patient has habit of eating paan since 25 yrs
SYSTEMIC EXAMINATION
SYSTEMIC EXAMINATION
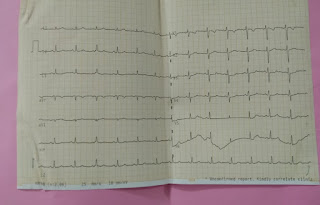
CARDIOVASCULAR SYSTEM
Inspection:
Chest wall is bilaterally symmetrical
No Precordial bulge
No visible pulsations, engorged veins,scars, sinuses
Palpation:
JVP - normal
Apex beat : felt in the left 6th intercostal space
Ausculation:
S1 ,S2 Heard












Provisional diagnosis :- Dilated cardiomyopathy, diabetic nephropathy and right pleural effusion with iron deficiency anemia


Comments
Post a Comment