This is an online e-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
A 60 yr old male patient presented to opd with chief complaints of altered sensorium (loss of consciousness) 5 days back and fever 5 days back and he had 1 episode of vomiting 6 days back
HISTORY OF PRESENT ILLNESS
Patient was apparently asymptomatic 15 yrs back
15 yrs back he had giddiness and weakness and on routine check up he was diagnosed as diabetes
then and 5 days back he presented to opd with chief complaint of altered sensorium 5 days back fever 5 days back and vomiting 6 days back
4 months back patient had injury to left foot small ulcer developed initially and then progressed and had amputation of last 3 toes of the foot
5 days back he went to party he had mutton curry he skipped taking medication then behaviour of patient was abnormal and had a episode of vomiting which is non bilious and non projectile
And since 15 yrs patient is on medication
PERSONAL HISTORY
Diet is mixed
Sleep is adequate
Bowel and bladder movements are regular
He has habit of alcohol consuming occasionally since 15 yrs continuously and since 5 months he consumes alcohol occassionally
FAMILY HISTORY
There is history of diabetes in the family members
PAST HISTORY
History of diabetes since 15 yrs and history of amputation of his left foot 4 months back
There is no history of hypertension, asthma; tuberculosis
GENERAL EXAMINATION:
Patient was concious coherent and coperative well oriented to time place and person.
- pallor
-No clubbing
-No cyanosis
-No icterus
-No generalized lymphedenopathy
-no pedal edema
VITALS
Temperature : febrile
Pulse rate: 78 beats per min
Respiratory rate : 24 cycles per min
Bp :110/ 80mm of Hg
Grbs - 524 mg/dl
Spo2 - 97% room air
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM
Inspection:
Chest wall is bilaterally symmetrical
No Precordial bulge
No visible pulsations, engorged veins,scars, sinuses
Palpation:
JVP - normal
Apex beat : felt in the left 5th intercostal space
In midclavicular line
Ausculation:
S1 ,S2 Heard
RESPIRATORY SYSTEM
Bilateral airway +
Position of trachea- central
Normal vesicular breaths heard
No added sounds
PER ABDOMEN
Abdomen is soft and non tender
Bowel sounds heard
No palpable mass or free fluid
CENTRAL NERVOUS SYSTEM
Patient is conscious
Reflexes are normal
Speech is normal

Amputation on his left foot last 3 toes
Fever chart
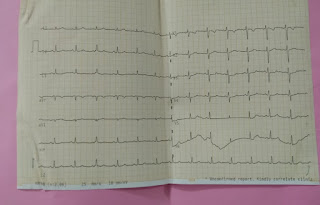
Investigations
Diagnosis :- Non ketotic hyperosmolar diabetic coma
Treatment













Comments
Post a Comment